
Maturity-Onset Diabetes of the Young (MODY) is a distinct, monogenic form of diabetes often misdiagnosed as Type 1 or Type 2 diabetes.
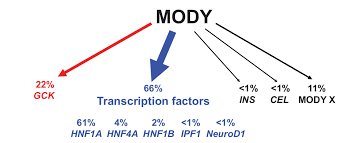
Among the genes implicated in MODY, HNF1A (Hepatocyte Nuclear Factor-1 Alpha) mutations are the most common cause of MODY3, the predominant subtype.
These mutations disrupt insulin secretion and glucose metabolism, leading to early-onset diabetes, often before age 25.
Understanding the role of HNF1A in beta-cell function and how its mutations contribute to MODY is critical for improving diagnosis and tailoring treatments.
In this article, BestDietarySupplementforDiabetics.com shall explore the “how” and “why” behind HNF1A mutations and their impact on MODY development.
From the gene’s role in insulin production to real-life case studies, we shall unravel the science step-by-step.
Article Index:
- What Causes MODY3 Diabetes?
- The Role of HNF1A in Glucose Regulation
- How HNF1A Mutations Affect Insulin Secretion
- Genetic Variants and Epigenetic Interactions in MODY3
- What is the Difference Between MODY and Type 1 Diabetes?
- Real-Life Case Study: Sarah’s Diagnosis of MODY3
- Best Treatment Options for HNF1A-Related MODY
- Impact of HNF1A Mutations on Pregnancy and Offspring
- Advances in Genetic Testing and Diagnosis
- FAQs on HNF1A Mutations and MODY
- How Lifestyle Factors Influence HNF1A Mutations
What Causes MODY3 Diabetes?
MODY3 results from autosomal dominant mutations in the HNF1A gene.
These mutations impair the transcription factor’s ability to regulate the genes involved in beta-cell function and glucose metabolism.
Unlike Type 1 diabetes, which involves autoimmune beta-cell destruction, or Type 2 diabetes, which is often linked to insulin resistance, MODY3 is characterized by a direct genetic cause.
HNF1A mutations disrupt the pancreatic beta cells’ ability to sense glucose levels and release insulin appropriately.
A study published in Nature Genetics highlights that MODY3 is the most common form of MODY, accounting for approximately 30-50% of all cases globally.
The Role of HNF1A in Glucose Regulation
HNF1A (Hepatocyte Nuclear Factor 1 Alpha) is a transcription factor predominantly expressed in the liver, kidneys, and pancreatic beta cells.
It plays a pivotal role in regulating genes essential for glucose metabolism.
Among its key functions, HNF1A oversees:
- Glucose Transport: It regulates the expression of glucose transporters like GLUT2, which are vital for glucose uptake by beta cells, enabling them to sense and respond to blood sugar levels.
- Insulin Secretion: By influencing genes responsible for glucose-sensing enzymes, HNF1A ensures that beta cells secrete sufficient insulin when blood glucose rises.
- Hepatic Glucose Production: It maintains balanced glucose production in the liver, preventing excessive glucose release into the bloodstream.
When HNF1A mutations occur, these finely tuned processes are disrupted, leading to impaired glucose sensing, insufficient insulin secretion, and dysregulated hepatic glucose output.
These dysfunctions are central to the development of MODY3, making HNF1A mutations a hallmark of this condition.
Understanding these mechanisms highlights the critical role of HNF1A in maintaining metabolic equilibrium.
How HNF1A Mutations Affect Insulin Secretion?
Mutations in HNF1A hinder its ability to bind DNA and activate gene transcription, resulting in:
- Defective Glucose Sensing: Reduced expression of glucose transporters leads to inadequate beta-cell glucose uptake.
- Impaired Insulin Production: The beta cells fail to secrete sufficient insulin, even in the presence of high blood glucose.
- Accelerated Beta-Cell Apoptosis: Chronic cellular stress induced by the mutations leads to early beta-cell death.
A study in The Journal of Clinical Endocrinology & Metabolism found that patients with HNF1A mutations exhibit higher fasting blood sugar levels and a progressive decline in beta-cell function, emphasizing the gene’s role in MODY development.
Genetic Variants and Epigenetic Interactions in MODY3
HNF1A mutations vary widely, with over 400 identified variants, including missense, nonsense, and frameshift mutations.
Each mutation impacts beta-cell function differently. For instance:
- Missense Mutations: Substitute one amino acid for another, altering protein function.
- Frameshift Mutations: Create a truncated, non-functional protein, severely disrupting glucose regulation.
Epigenetics adds another layer of complexity. Maternal glucose levels during pregnancy can influence gene expression in the fetus, further increasing the risk of developing MODY3 later in life.
This interplay between genes and the environment illustrates why MODY is often familial but variably expressed.
What is the Difference Between MODY and Type 1 Diabetes?
MODY (Maturity-Onset Diabetes of the Young) is frequently misdiagnosed as Type 1 diabetes due to its early onset during adolescence or young adulthood.
However, several critical differences help differentiate the two conditions:
- Genetic Basis: MODY arises from a single gene mutation (monogenic), such as HNF1A mutations in MODY3. In contrast, Type 1 diabetes is polygenic and involves an autoimmune attack on insulin-producing beta cells.
- Insulin Dependence: Unlike Type 1 diabetes, where insulin therapy is essential from the outset, most MODY cases, including MODY3, do not require insulin initially. Instead, they often respond effectively to oral medications like sulfonylureas, which stimulate insulin secretion.
- Family History: MODY follows an autosomal dominant inheritance pattern, meaning it often appears in multiple generations within a family. This inheritance pattern makes family history a valuable diagnostic clue, as opposed to the sporadic occurrence of Type 1 diabetes.
Recognizing these distinctions is crucial to avoid unnecessary insulin therapy and to provide the most effective management strategies for individuals with MODY.
Real-Life Case Study: Sarah’s Diagnosis of MODY3
Sarah, a 26-year-old nurse, struggled with fluctuating blood sugar levels despite a healthy lifestyle.
Her father, diagnosed with diabetes in his 30s, encouraged her to undergo genetic testing. The results confirmed an HNF1A mutation.
Sarah’s diagnosis clarified her condition: MODY3, not Type 2 diabetes. Her endocrinologist prescribed sulfonylureas, which improved her glucose control significantly.
This case underscores the importance of genetic testing for atypical diabetes presentations, particularly in young patients with a strong family history.
Best Treatment Options for HNF1A-Related MODY
MODY3 patients benefit from sulfonylureas, which stimulate insulin release by bypassing the glucose-sensing defects caused by HNF1A mutations.
Unlike insulin therapy, sulfonylureas directly address the underlying pathophysiology.
Studies suggest that early intervention with these medications can slow beta-cell deterioration, improving long-term outcomes.
While insulin may be required in advanced cases, most patients with MODY3 achieve effective glucose control with oral medications.
Impact of HNF1A Mutations on Pregnancy and Offspring
HNF1A mutations don’t just affect the individual—they can significantly influence pregnancy outcomes and the health of offspring.
These mutations often lead to maternal hyperglycemia, which has a profound impact on fetal beta-cell function.
This exposure can predispose the child to glucose dysregulation later in life, increasing the risk of conditions like impaired glucose tolerance or diabetes.
The question arises: Can HNF1A mutations cause complications during pregnancy?
The answer is yes. Poorly controlled blood sugar in pregnant individuals with HNF1A mutations heightens the risk of complications such as macrosomia (large birth weight) and neonatal hypoglycemia, where the newborn experiences dangerously low blood sugar levels shortly after birth.
Effective management of maternal glucose levels is crucial to minimize these risks.
A study in Diabetes Care emphasizes the importance of monitoring blood sugar closely during pregnancy and tailoring treatment to the unique challenges posed by MODY3, ensuring better outcomes for both mother and baby.
FAQs on HNF1A Mutations and MODY
Q-1: How do HNF1A gene mutations cause MODY3 diabetes?
A-1: Mutations in the HNF1A gene impair the function of a key transcription factor that regulates insulin production in pancreatic beta cells.
This leads to reduced insulin secretion, resulting in a form of monogenic diabetes known as Maturity-Onset Diabetes of the Young, specifically MODY3.
In the U.S., MODY accounts for about 1–2% of all diabetes cases, though it is often underdiagnosed.
Q-2: What is the role of HNF1A in beta-cell function?
A-2: HNF1A controls genes involved in glucose sensing and insulin secretion. When mutated, beta cells lose their ability to respond effectively to rising blood glucose levels. This dysfunction leads to progressive hyperglycemia over time.
Q-3: What are the symptoms of HNF1A-MODY?
A-3: Symptoms often appear in adolescence or early adulthood and include:
- Mild to moderate high blood sugar
- Excessive thirst and urination
- Family history of early-onset diabetes
Unlike Type 1 Diabetes, patients usually do not require immediate insulin therapy at diagnosis.
Q-4: How do HNF1A mutations affect insulin secretion pathways?
A-4: These mutations disrupt gene expression in beta cells, reducing glucose transport and insulin release. As a result, the pancreas produces insulin but cannot secrete enough in response to meals.
Q-5: What is the difference between HNF1A-MODY and Type 2 diabetes?
A-5: While Type 2 Diabetes is primarily driven by insulin resistance, HNF1A-MODY is caused by a genetic defect in insulin secretion. Patients with MODY are typically younger, leaner, and have a strong family history of diabetes.
Q-6: How is HNF1A-MODY diagnosed in the U.S.?
A-6: Diagnosis involves genetic testing to identify mutations in the HNF1A gene. The American Diabetes Association recommends considering MODY in individuals with early-onset diabetes and a strong family history. Genetic testing is becoming more accessible but remains underutilized.
Q-7: How common are HNF1A mutations in monogenic diabetes?
A-7: HNF1A mutations are among the most common causes of MODY, accounting for 30–50% of cases. However, many cases are misdiagnosed as type 1 or type 2 diabetes, leading to inappropriate treatment.
Q-8: What are the treatment options for HNF1A-MODY?
A-8: Patients respond well to low-dose sulfonylureas, which stimulate insulin secretion. Unlike other forms of diabetes, many individuals can avoid insulin therapy for years. Personalized treatment is key.
Q-9: What are the clinical features of MODY3 caused by HNF1A mutation?
A-9:
- Early onset (before age 25)
- Progressive beta-cell dysfunction
- Sensitivity to sulfonylurea drugs
- Autosomal dominant inheritance
These features distinguish it from other diabetes types.
Q-10: What is the inheritance pattern of HNF1A-MODY?
A-10: HNF1A-MODY follows an autosomal dominant inheritance pattern, meaning a child has a 50% chance of inheriting the mutation if one parent is affected. Family screening is crucial for early detection.
Q-11: How do HNF1A variants influence age of diabetes onset?
A-11: Different mutations can affect how early symptoms appear. Some variants lead to diabetes in adolescence, while others may delay onset until adulthood. Environmental factors like diet and lifestyle can also influence progression.
Q-12: What is the pathophysiology of HNF1A mutation in pancreatic beta cells?
A-12: The mutation disrupts transcriptional regulation of genes involved in glucose metabolism. This leads to reduced insulin synthesis and secretion, causing chronic hyperglycemia. Over time, beta-cell function continues to decline.
U.S. Statistics You Should Know:
- Over 37 million Americans have diabetes
- MODY represents 1–2% of all diabetes cases
- Up to 80% of MODY cases are misdiagnosed
- Early diagnosis can significantly improve treatment outcomes
(Source: Centers for Disease Control and Prevention)
Actionable Clinical Insights
- Consider genetic testing if diabetes appears before age 25 with family history
- Avoid misdiagnosis: MODY patients often don’t need insulin initially
- Use targeted therapy: Sulfonylureas are highly effective
- Screen family members due to hereditary risk
- Monitor progression: Regular glucose and HbA1c checks are essential
Why Accurate Diagnosis Matters?
Misdiagnosing HNF1A-MODY as type 1 or type 2 diabetes can lead to unnecessary insulin use or ineffective treatment. Precision medicine—tailoring treatment based on genetic diagnosis—is transforming diabetes care in the U.S.
Free Tip for the Day:
HNF1A mutations play a central role in the development of MODY3 by directly impairing insulin secretion at the genetic level. Although relatively rare, this condition is significantly underdiagnosed and often mistaken for more common forms of diabetes.
In a country like the U.S., where diabetes prevalence is high, improving awareness of monogenic diabetes is essential. Early genetic testing, accurate diagnosis, and targeted treatment can dramatically improve patient outcomes.
Ultimately, understanding the genetic roots of diabetes not only refines treatment strategies but also highlights the growing importance of personalized medicine in modern healthcare.
Advances in Genetic Testing and Diagnosis
Genetic testing has become the definitive approach for diagnosing MODY, especially MODY3 caused by HNF1A mutations.
Advances in sequencing technologies, such as next-generation sequencing (NGS) panels, allow for precise and efficient identification of genetic variants linked to the condition.
Early diagnosis through genetic testing offers several advantages:
- Tailored Treatment: Identifying the exact mutation enables healthcare providers to recommend appropriate treatments, such as sulfonylureas, over standard diabetes management strategies.
- Avoiding Misdiagnosis: Genetic testing differentiates MODY3 from Type 1 or Type 2 diabetes, reducing unnecessary insulin prescriptions and avoiding the complications of mismanagement.
- Cascade Testing: Once a mutation is identified, family members can undergo testing to assess their risk, enabling early intervention if necessary.
Patients often wonder, “How does genetic testing diagnose MODY?” The answer lies in its ability to pinpoint specific mutations that disrupt glucose regulation, providing clarity for both diagnosis and treatment.
How Lifestyle Factors Influence HNF1A Mutations?
While HNF1A mutations form the genetic basis of MODY3, environmental factors such as diet and exercise significantly influence its development and progression.
Poor lifestyle choices, including high-calorie diets and sedentary behavior, can worsen the effects of these mutations by increasing insulin resistance and placing additional stress on pancreatic beta cells.
This interplay between genetics and environment raises the question, “Why is MODY3 the most common MODY type?”
One possible explanation lies in how prevalent lifestyle factors, such as unhealthy eating and limited physical activity, amplify the metabolic challenges posed by HNF1A mutations.
These environmental triggers may contribute to its higher occurrence compared to other MODY types.
The good news is that addressing these factors can positively impact disease management.
Studies have shown that adopting a balanced diet and engaging in regular exercise not only improve glucose control but also help delay the progression of MODY3.
Conclusion
HNF1A mutations significantly influence MODY development by impairing beta-cell function and disrupting glucose metabolism.
Understanding the genetic and epigenetic mechanisms involved allows for precise diagnosis and treatment, ensuring better outcomes for patients.
Through genetic testing, personalized treatment plans, and lifestyle modifications, individuals with MODY3 can achieve effective glucose control and a better quality of life.
By integrating advanced research and clinical care, the future looks promising for those affected by HNF1A mutations.
Recommended:
- https://pmc.ncbi.nlm.nih.gov/articles/PMC8948720/
- https://bestdietarysupplementfordiabetics.com/how-air-pollution-impacts-mody-diabetes-development/
- https://bestdietarysupplementfordiabetics.com/how-hnf4a-mutations-lead-to-impaired-insulin-secretion/
- https://bestdietarysupplementfordiabetics.com/how-hnf1b-mutations-impair-insulin-production/
- why trust us?
- for educational purpose only
admin
All Posts