
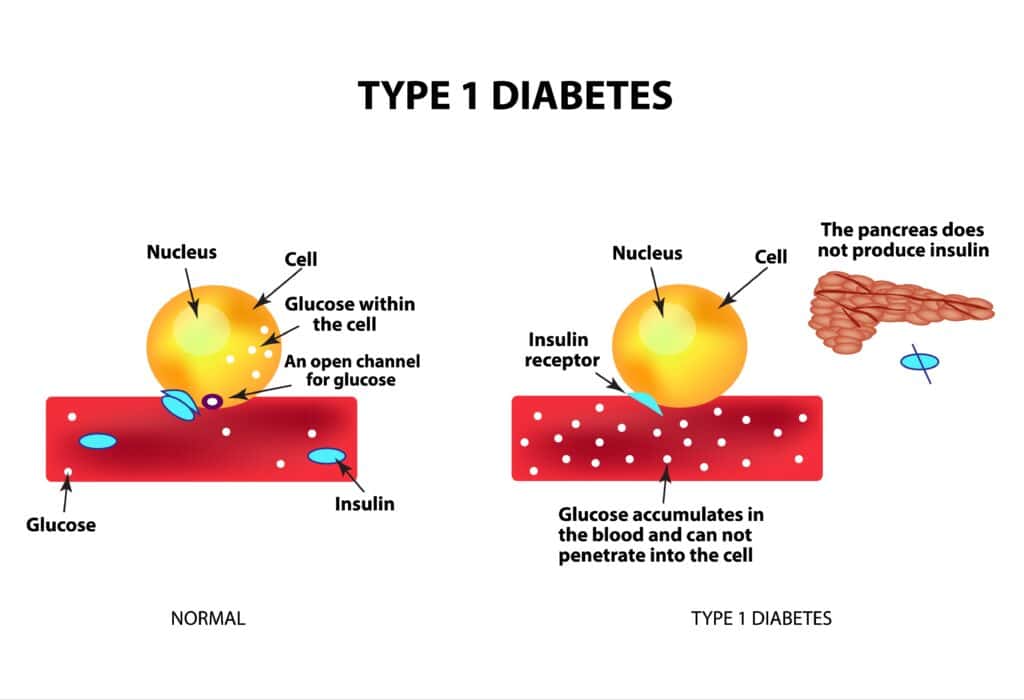
Type 1 diabetes (T1D) is a chronic autoimmune condition in which the body’s immune system mistakenly attacks and destroys insulin-producing beta cells in the pancreas.
Unlike type 2 diabetes, which is largely influenced by lifestyle and metabolic factors, type 1 diabetes is primarily driven by genetic susceptibility and immune dysfunction.
Among the many genes studied in connection with this disease, the Human Leukocyte Antigen (HLA) region has been identified as the most important genetic contributor.
Within this region, the HLA-DR gene plays a particularly significant role in determining whether an individual develops autoimmune diabetes.
The HLA-DR gene influences how immune cells recognize and respond to proteins in the body. Certain variants of this gene, especially HLA-DR3 and HLA-DR4, are strongly associated with an increased risk of developing type 1 diabetes.
These variants can alter the way immune cells interpret pancreatic proteins, causing them to be mistakenly recognized as foreign threats.
Once this immune misidentification occurs, a chain reaction begins in which immune cells attack the insulin-producing beta cells.
Over time, this autoimmune attack gradually reduces the pancreas’s ability to produce insulin. When a large percentage of beta cells are destroyed, blood sugar levels begin to rise and the clinical symptoms of diabetes appear.
As per bestdietarysupplementfordiabetics.com, “Understanding the role of the HLA-DR gene is therefore essential for explaining why some people develop type 1 diabetes while others do not, even when they share similar environmental exposures”.
Article Index
- Understanding the Human Leukocyte Antigen (HLA) System
- What Is the HLA-DR Gene?
- Location of the HLA-DR Gene in the Human Genome
- How HLA-DR Genes Influence Immune Recognition
- High-Risk HLA-DR Variants Associated With Type 1 Diabetes
- Step-by-Step Mechanism of Autoimmune Beta Cell Destruction
- Role of HLA-DR3 and HLA-DR4 in Type 1 Diabetes Development
- Statistical Evidence Linking HLA-DR Genes to Diabetes Risk
- Protective HLA Variants That Lower Diabetes Risk
- Genetic Screening and Future Research on HLA-DR
- FAQ: HLA-DR Gene and Type 1 Diabetes
Understanding the Human Leukocyte Antigen (HLA) System
The Human Leukocyte Antigen (HLA) system is a complex group of genes that regulate immune responses in the human body.
These genes help the immune system distinguish between the body’s own cells and foreign substances such as viruses, bacteria, and other pathogens.
HLA genes produce specialized proteins that sit on the surface of many cells in the body. These proteins act like display platforms that present small fragments of proteins, called antigens, to immune cells.
Once these fragments are displayed, immune cells decide whether the protein is harmless or whether it represents a threat that must be eliminated.
The HLA system is divided into three main groups:
- HLA Class I genes
• HLA Class II genes
• HLA Class III genes
Type 1 diabetes is most strongly associated with HLA Class II genes, particularly HLA-DR and HLA-DQ. These genes regulate the activity of helper T-cells, which coordinate immune responses.
Because the HLA system is highly variable between individuals, different people respond differently to infections and immune triggers.
This genetic diversity helps protect populations against a wide range of diseases. However, certain HLA variations can increase susceptibility to autoimmune disorders, including type 1 diabetes.
What Is the HLA-DR Gene?
The HLA-DR gene belongs to the HLA Class II gene family and plays an important role in immune communication. It produces proteins that help present antigens to CD4+ helper T-cells, which regulate immune responses.
Each HLA-DR molecule is composed of two protein chains:
- An alpha chain
• A beta chain
The beta chain, encoded by the HLA-DRB1 gene, is highly variable and determines how antigens bind to the receptor. Even small genetic differences in this region can significantly affect how the immune system recognizes proteins.
When certain HLA-DR variants bind fragments of pancreatic beta-cell proteins, these fragments may be presented to immune cells as if they were harmful. This abnormal presentation can trigger an immune response against insulin-producing cells.
As a result, the immune system begins attacking the pancreas, leading to the gradual destruction of beta cells and the development of type 1 diabetes.
Location of the HLA-DR Gene in the Human Genome
The HLA-DR gene is located within the Major Histocompatibility Complex (MHC) on chromosome 6. This region contains a large cluster of genes that regulate immune function.
The MHC region is one of the most genetically diverse areas of the human genome. This diversity allows the immune system to recognize a wide variety of pathogens and respond effectively to infections.
Within this region, the HLA-DR gene cluster typically includes several related genes, such as:
- DRB1
• DRB3
• DRB4
• DRB5
These genes produce slightly different versions of HLA-DR proteins. Each version is capable of presenting different antigen fragments to immune cells.
Because individuals inherit HLA genes from both parents, they often carry multiple HLA-DR variants.
The specific combination of these genes forms an HLA haplotype, which plays a major role in determining a person’s risk for autoimmune diseases.
How HLA-DR Genes Influence Immune Recognition?
The immune system relies on antigen presentation to determine whether to activate a defensive response. HLA-DR molecules are central to this process because they present protein fragments to helper T-cells.
During a normal immune response, HLA-DR molecules display fragments from invading microbes. Helper T-cells then activate other immune cells to eliminate the infection.
However, certain HLA-DR variants can present fragments of the body’s own proteins in a way that appears abnormal to the immune system.
In type 1 diabetes, these fragments often originate from proteins found in pancreatic beta cells.
When these proteins are presented incorrectly, helper T-cells may interpret them as foreign threats.
This mistaken recognition initiates an autoimmune response in which immune cells begin attacking the pancreas.
Over time, repeated immune attacks cause inflammation in pancreatic islets and gradual destruction of insulin-producing cells.
High-Risk HLA-DR Variants Associated With Type 1 Diabetes
Certain variants of the HLA-DR gene significantly increase the risk of developing type 1 diabetes.
The most important high-risk variants include:
- HLA-DR3
• HLA-DR4
Individuals who carry either of these variants have a higher probability of developing autoimmune diabetes compared with the general population.
The risk increases even further when a person inherits both HLA-DR3 and HLA-DR4. This combination creates a stronger immune response against pancreatic proteins and greatly increases susceptibility to beta-cell autoimmunity.
Children who carry this high-risk genetic combination are more likely to develop early immune markers of diabetes, such as autoantibodies targeting pancreatic cells.
Step-by-Step Mechanism of Autoimmune Beta Cell Destruction
The development of type 1 diabetes usually occurs through a gradual autoimmune process. The HLA-DR gene influences several key stages in this process.
Step 1 – Genetic predisposition:
An individual inherits high-risk HLA-DR variants from one or both parents.
Step 2 – Environmental trigger:
Factors such as viral infections, immune stress, or environmental exposures activate the immune system.
Step 3 – Antigen presentation:
HLA-DR molecules present fragments of pancreatic proteins to helper T-cells.
Step 4 – Immune activation:
Helper T-cells activate cytotoxic T-cells and B-cells that begin targeting pancreatic tissue.
Step 5 – Autoantibody production:
The immune system produces antibodies against insulin and other beta-cell proteins.
Step 6 – Beta-cell destruction:
Immune cells infiltrate the pancreatic islets and gradually destroy insulin-producing cells.
Step 7 – Clinical diabetes:
When most beta cells are destroyed, the pancreas can no longer produce sufficient insulin, leading to high blood sugar and the symptoms of diabetes.
Role of HLA-DR3 and HLA-DR4 in Type 1 Diabetes Development
Two HLA variants dominate the genetic risk for type 1 diabetes: HLA-DR3 and HLA-DR4. These genes influence immune responses in slightly different ways.
HLA-DR3 is associated with increased recognition of insulin-related proteins by helper T-cells. This increases the likelihood that the immune system will react to insulin-producing cells.
When both genes are present together, the immune system becomes highly reactive to pancreatic antigens. This greatly increases the likelihood of autoimmune destruction of beta cells.
Statistical Evidence Linking HLA-DR Genes to Diabetes Risk
Large genetic studies have shown that the HLA region contributes a major portion of the genetic susceptibility to type 1 diabetes.
Research indicates that HLA genes account for roughly 40–50 percent of the inherited risk associated with this disease. This makes them the most influential genetic factor identified in autoimmune diabetes.
High-risk HLA combinations are particularly common in individuals diagnosed with type 1 diabetes during childhood or adolescence. Many of these individuals carry the DR3, DR4, or DR3/DR4 genetic pattern.
However, only a small percentage of people with these genes actually develop diabetes. This shows that genetics alone cannot fully explain the disease and that environmental influences also play an important role.
Protective HLA Variants That Lower Diabetes Risk
While some HLA genes increase susceptibility to autoimmune diabetes, others appear to provide protection.
Protective variants improve the immune system’s ability to distinguish between self-proteins and foreign antigens. As a result, autoreactive immune cells are eliminated before they can attack the body’s tissues.
This protective mechanism strengthens immune tolerance, which prevents the immune system from attacking healthy cells.
Individuals carrying these protective variants rarely develop type 1 diabetes, even if other risk factors are present.
Genetic Screening and Future Research on HLA-DR
Advances in genetics have made it possible to identify individuals at high risk of developing type 1 diabetes through genetic screening.
Modern research programs analyze combinations of:
- HLA-DR genes
• HLA-DQ genes
• Diabetes-related autoantibodies
Children with high-risk genetic profiles can be monitored for early immune changes long before the onset of symptoms.
Researchers are also investigating therapies that could interrupt the autoimmune process before significant beta-cell destruction occurs.
Future scientific developments may lead to early prevention strategies, personalized genetic risk assessments, and immune-modulating therapies that delay or prevent diabetes.
FAQ: HLA-DR Gene and Type 1 Diabetes
Q-1: How does the HLA-DR gene cause type 1 diabetes?
A-1: The HLA-DR gene influences how the immune system identifies proteins in the body. Certain variants of this gene present fragments of pancreatic beta-cell proteins to immune cells.
When these proteins are mistakenly recognized as harmful, the immune system begins attacking the insulin-producing beta cells. Over time, this autoimmune response destroys the cells responsible for insulin production, eventually leading to type 1 diabetes.
Q-2: What is the role of HLA-DR3 and HLA-DR4 in type 1 diabetes?
A-2: HLA-DR3 and HLA-DR4 are two genetic variants strongly associated with an increased risk of type 1 diabetes. Individuals who inherit either of these genes are more likely to develop autoimmune reactions against pancreatic beta cells.
The risk becomes significantly higher when both variants are present together because this combination increases immune sensitivity toward insulin-producing cells.
Q-3: Why do HLA genes increase the risk of autoimmune diabetes?
A-3: HLA genes regulate antigen presentation, which determines how immune cells detect threats in the body. Some HLA variants present fragments of the body’s own proteins in a way that appears abnormal to immune cells.
This mistaken recognition can trigger an autoimmune response in which the immune system attacks healthy tissues, including the insulin-producing cells of the pancreas.
Q-4: Which HLA genotype has the highest risk for type 1 diabetes?
A-4: The highest genetic risk occurs in individuals who carry the HLA-DR3/DR4 combination. This genotype increases the likelihood that pancreatic proteins will be presented to immune cells in a way that triggers autoimmune activity.
Q-5: Where is the HLA-DR gene located in the human genome?
A-5: The HLA-DR gene is located on chromosome 6 within a region known as the major histocompatibility complex. This region contains several genes responsible for regulating immune responses and antigen presentation.
Q-6: Can someone develop type 1 diabetes without high-risk HLA genes?
A-6: Yes. Although HLA genes play a major role, type 1 diabetes is influenced by multiple factors. Other genes, environmental triggers, viral infections, and immune abnormalities can also contribute to the development of the disease.
Q-7: What immune cells are activated by HLA-DR genes in diabetes?
A-7: HLA-DR molecules activate CD4+ helper T-cells, which coordinate immune responses. These cells stimulate other immune cells such as cytotoxic T-cells and B-cells that attack pancreatic beta cells.
Q-8: How common are high-risk HLA genes in people with type 1 diabetes?
A-8: A large proportion of individuals with type 1 diabetes carry high-risk HLA variants, particularly HLA-DR3 or HLA-DR4. Many patients possess one or both of these genes, which explains why the HLA region is considered the most important genetic factor in autoimmune diabetes.
Q-9: Can genetic testing detect HLA-DR risk for diabetes?
A-9: Yes. Genetic tests can identify specific HLA-DR variants associated with increased risk of type 1 diabetes. These tests can help researchers and clinicians identify individuals who may be genetically susceptible to the disease.
Q-10: Can understanding the HLA-DR gene help prevent type 1 diabetes?
A-10: Understanding how HLA-DR genes influence immune responses helps researchers detect early autoimmune activity. This knowledge is guiding the development of preventive strategies aimed at stopping immune attacks before significant pancreatic damage occurs.
Conclusion
The HLA-DR gene plays a central role in the development of type 1 diabetes by influencing how the immune system recognizes proteins in the body.
Located within the immune-regulating HLA region on chromosome 6, this gene produces molecules responsible for presenting antigens to helper T-cells.
Certain genetic variants, particularly HLA-DR3 and HLA-DR4, can alter the way pancreatic proteins are presented to immune cells.
When these proteins are mistakenly recognized as foreign, the immune system launches an attack against insulin-producing beta cells.
Over time, this autoimmune process gradually destroys the pancreas’s ability to produce insulin, leading to the onset of diabetes.
Although the HLA-DR gene accounts for a large portion of the genetic risk, it does not act alone.
Environmental triggers and other genes also influence whether the disease develops.
Continued research into HLA genetics is helping scientists better understand autoimmune diabetes and may eventually lead to improved screening methods, preventive therapies, and more effective treatments for people at risk.
Recommended:
- https://bestdietarysupplementfordiabetics.com/how-hla-dq-gene-causes-type-1-diabetes/
- https://diabetesjournals.org/care/article/48/2/202/157547/Genetic-Discovery-and-Risk-Prediction-for-Type-1
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10659516/
- Why trust bestdietarysupplementfordiabetics.com?
- For educational purpose only
admin
All Posts